RECIST 1.1.
Plus the depth
it can't give you.
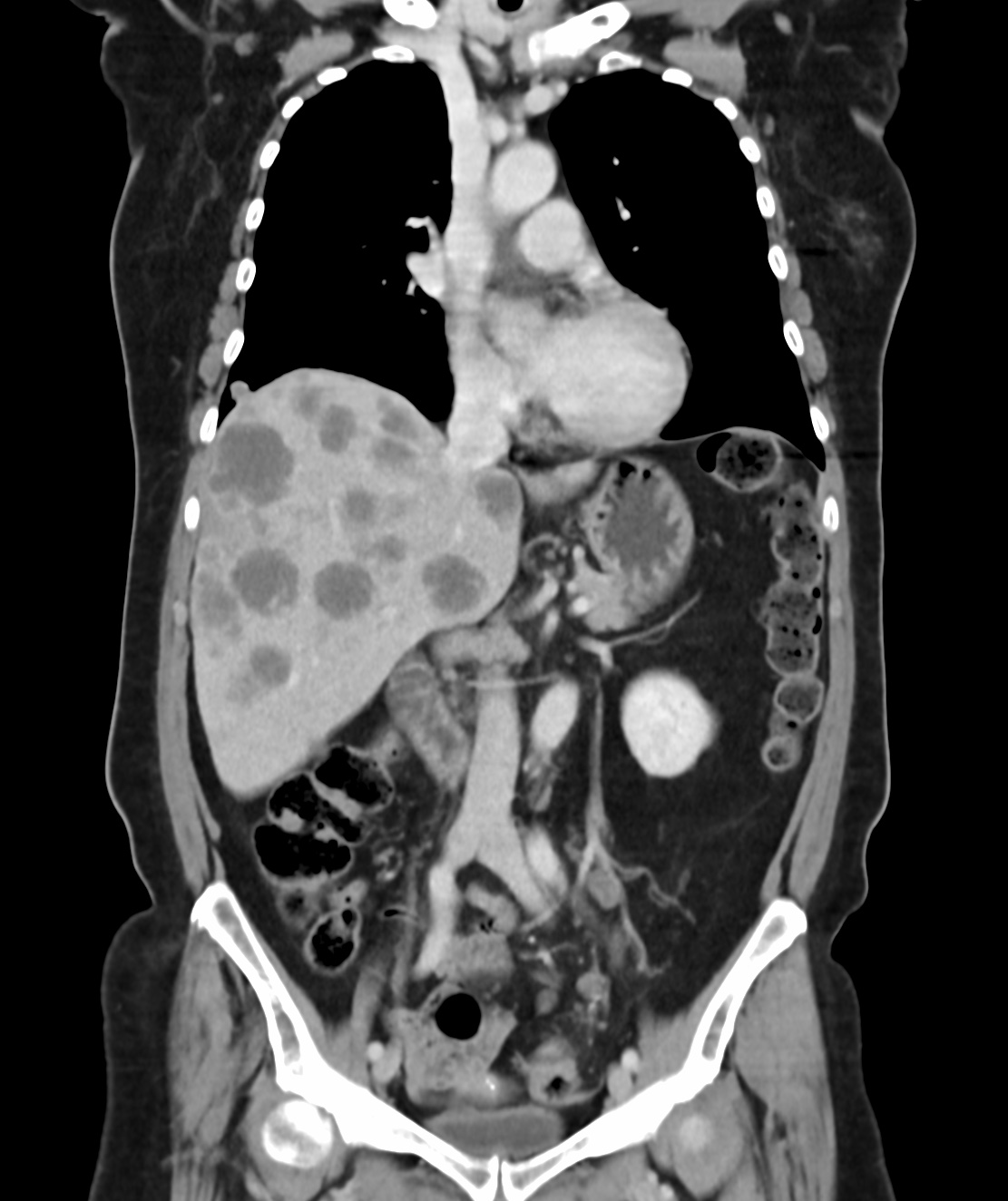
CE CT · Portal Venous Phase
Organ-Specific Lesions Tracking
Clinical Context
Longest diameter stays stable while the tumor hollows out. Viable volume may be dropping 40–60% — a signal RECIST cannot capture.
Cavitation3 mm shrinkage → 65.5 cm³ → 54.4 cm³ (−17% volume). 3 mm growth → 65.5 cm³ → 78.0 cm³ (+19% volume). RECIST rounds off your tumor's biology.
ResolutionA shrinking liver met plus a growing lung lesion yields apparent SD. Per-site volumetric mapping shows you which organ system is failing.
Mixed ResponseSupported Criteria
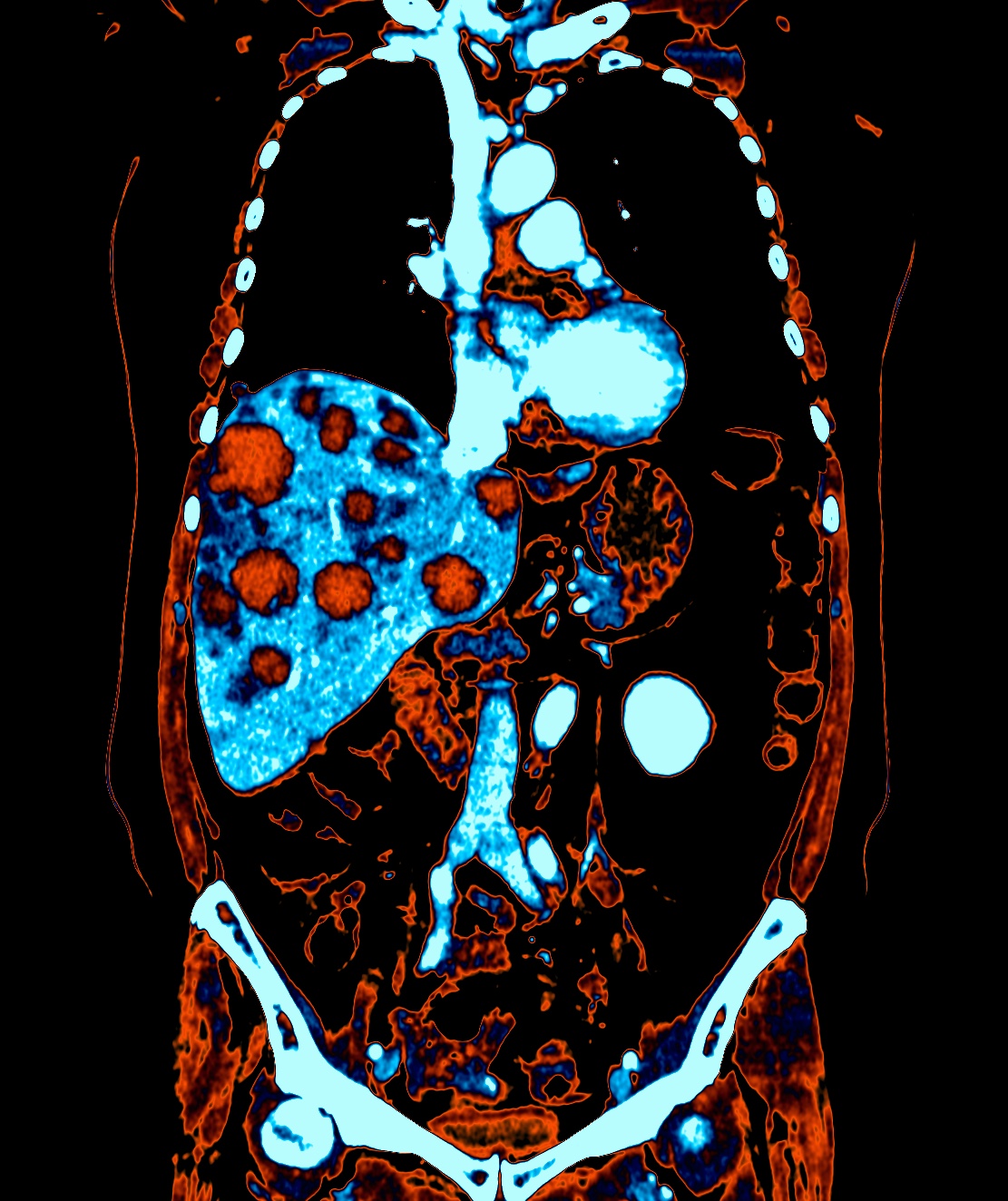
Beyond RECIST

Viable tumor (red) vs. parenchyma (blue) tracked across sequential slices. Same images as RECIST read — no additional scan required.
Full-Stack Imaging
Automated slice thickness, contrast protocol, and timing verification. Every study validated before it enters the read queue — preventing late-stage rejects that delay database lock.
Independent BICR by solid tumor-trained radiologists. 24–72h turnaround per timepoint, results in BioSUITE dashboard, third-reader adjudication built in. Full audit trail for 21 CFR Part 11.
3D tumor volume, viable tissue separation, ΔVolume trending, and per-site response mapping — delivered in BioSUITE, not a separate engagement. Available 24–72h after image receipt.
Why Volumetryx
3D volume, viable tissue, ΔVolume — in every solid tumor engagement. No surprises, no scope-change conversations mid-trial.
Decision-critical data when the decision is being made — not batched quarterly in a summary PDF.
Raw measurements, segmentation files, volumetric data in CSV/JSON. No data hostage situations at contract renewal.
RECIST 1.1, iRECIST, irRECIST, irRC, mRECIST — same platform, same team. No criteria gaps, no vendor switching.

Tell us your criteria, modality, and number of sites. We'll scope it within 48 hours.