Quantitative Imaging
What We Measure in mCRPC
Mean PSMA uptake across all quantified tumor.
The single strongest multivariate predictor of PSA response and overall survival after 177Lu-PSMA. Threshold enrichment: SUVmean ≥10. Validated across VISION, TheraP, taxane chemotherapy, and the U.S. Expanded Access Program. Unavailable from a qualitative read.
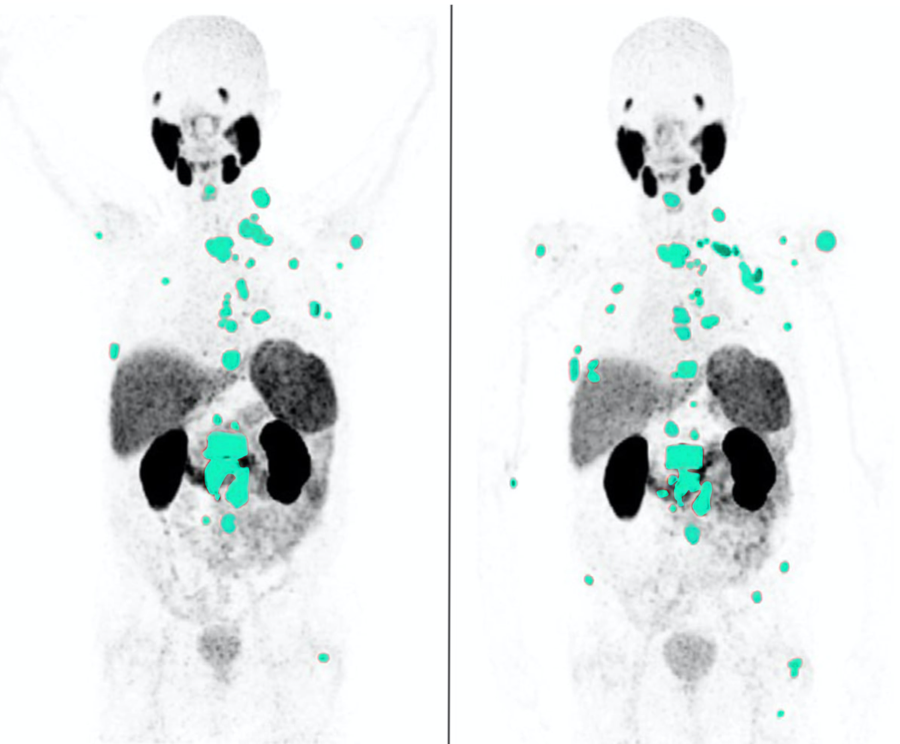
Whole-body volume of PSMA-avid disease.
Segmented across all lesions using a threshold derived from liver or blood-pool uptake. The quantitative input RECIP 1.0 requires to assign CR / PR / SD / PD. Called PSMA-VOL by Gafita and TTV in later literature — same parameter, two conventions.
Longitudinal percent change from baseline.
Applied directly against RECIP 1.0 cutoffs: ≥30% decrease with no new lesions = PR, ≥20% increase with new lesions = PD. Calculated per patient at each scheduled timepoint. Cannot be reconstructed retroactively from a narrative read.
PSMA-VOL ÷ SUVmean. Volume multiplied by expression.
Composite prognostic biomarker — tumor burden weighted by PSMA intensity. Independently prognostic for OS in mCRPC across multiple cohorts. Directly analogous to TLG in FDG-PET. Stable across software platforms and reconstructions.