RANO 2.0 Validated
Volumetric Endpoints.
We Run Volumetry.
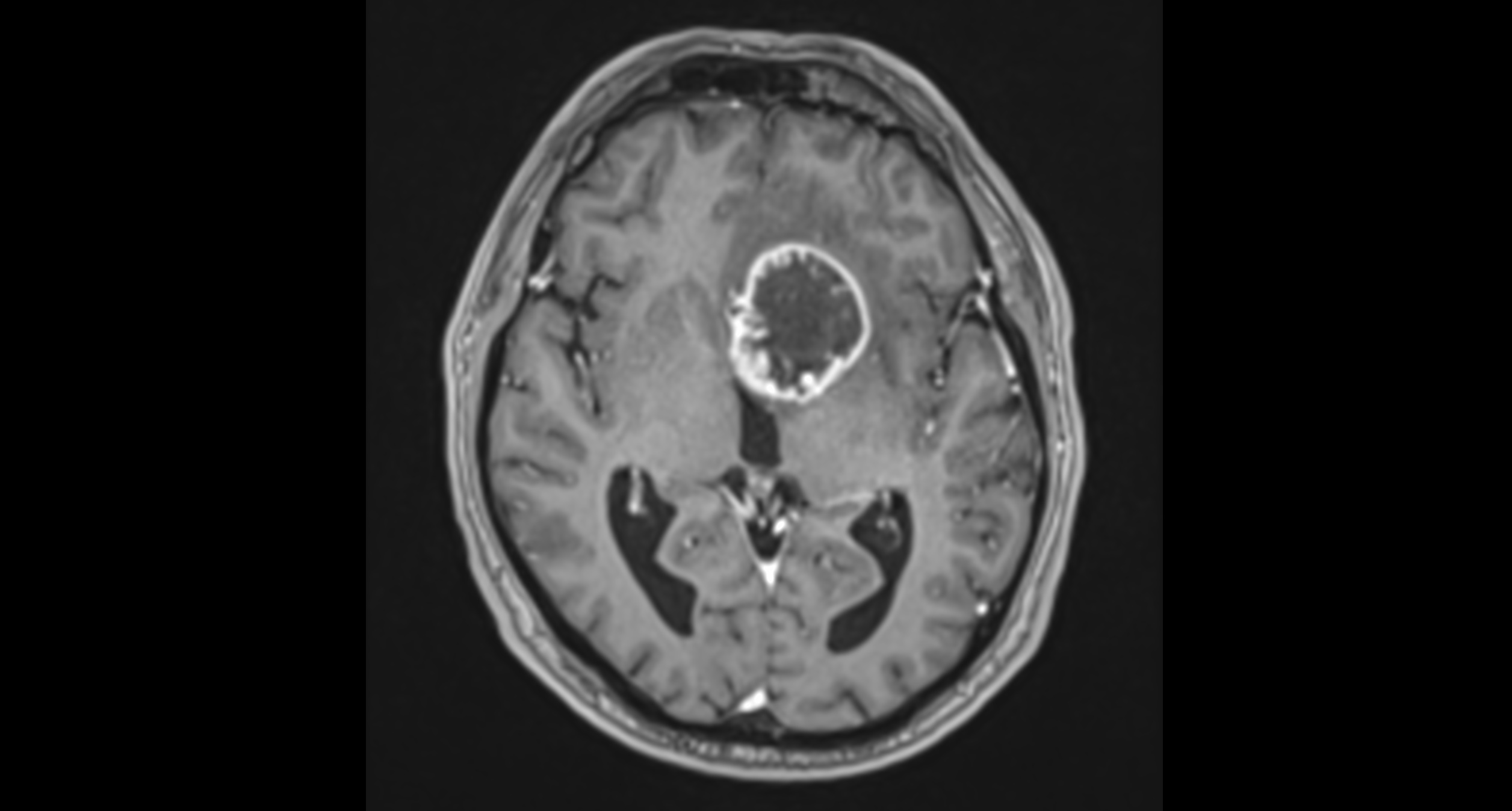
T1 MRI
Volumetric Segmentation
Clinical Challenge
But the reader picks a slice one position off — a different cross-section of an irregular 3D mass. The apparent diameter changes by 2 mm in one axis. The bidimensional product swings 15–20% on the same scan, same day, same lesion. Next timepoint, a different reader picks a different slice. Your trend is noise.
Place the calipers 0.5 mm off on the same slice and it's worse: D1 over-read, D2 under-read, errors partially cancel. Or D1 and D2 both over-read because the reader included meningeal thickening — errors compound. You don't know which one happened. Neither does the biostatistician analyzing your PFS.
Volumetric segmentation uses every slice. Boundary errors distribute across thousands of surface voxels and average out. The trend holds across timepoints — even across readers.
Three timepoints of +12% / +28% / +15% by 2D tells you nothing.
Three timepoints of +31% / +33% / +35% by volume tells you progression is building.
RANO 2.0 codified volumetric thresholds. The operational guide recommends consistent software across all patients in multicenter trials. We deliver exactly that.
Measurement PrecisionSupported Criteria
Quantitative Imaging
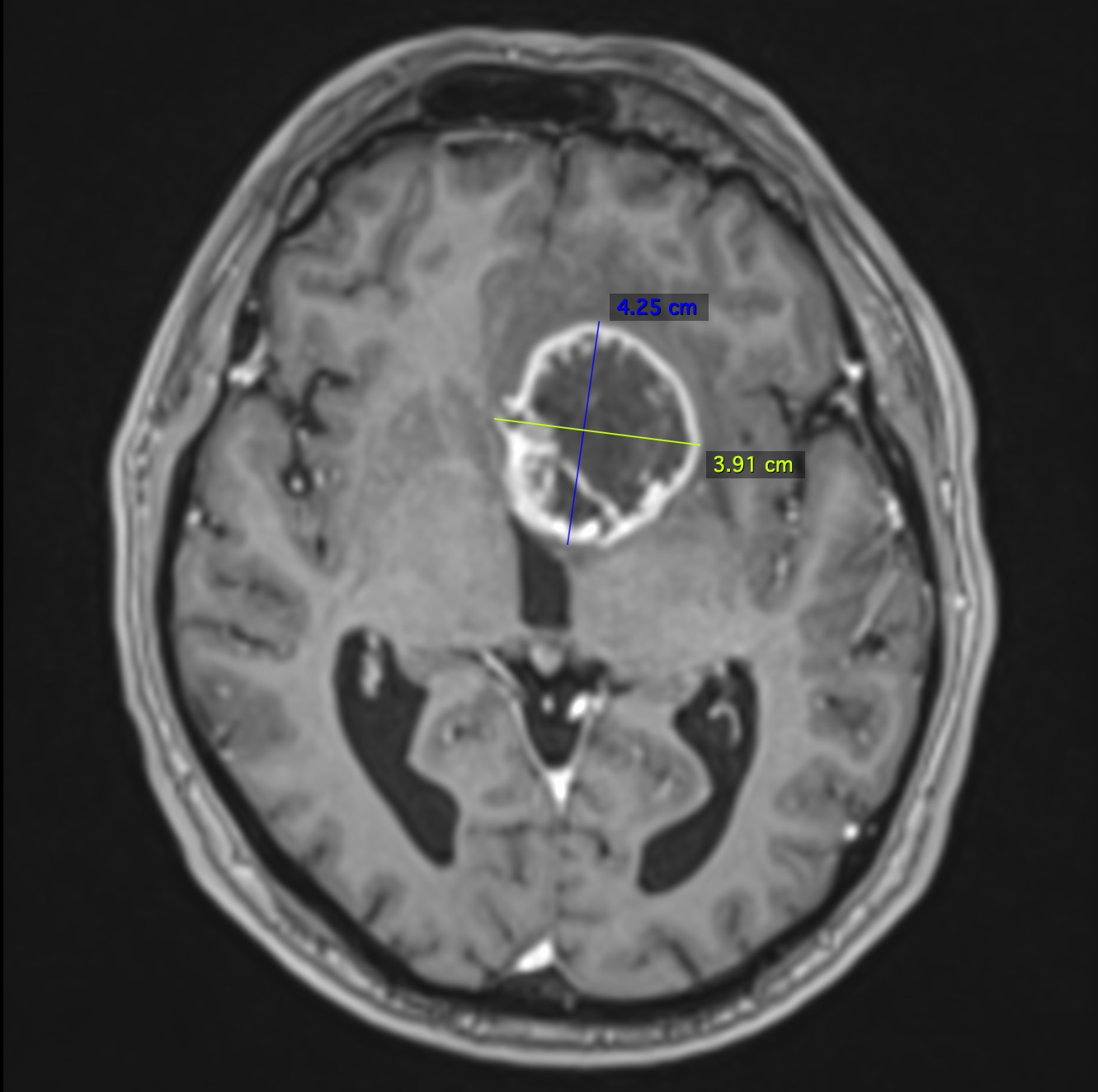
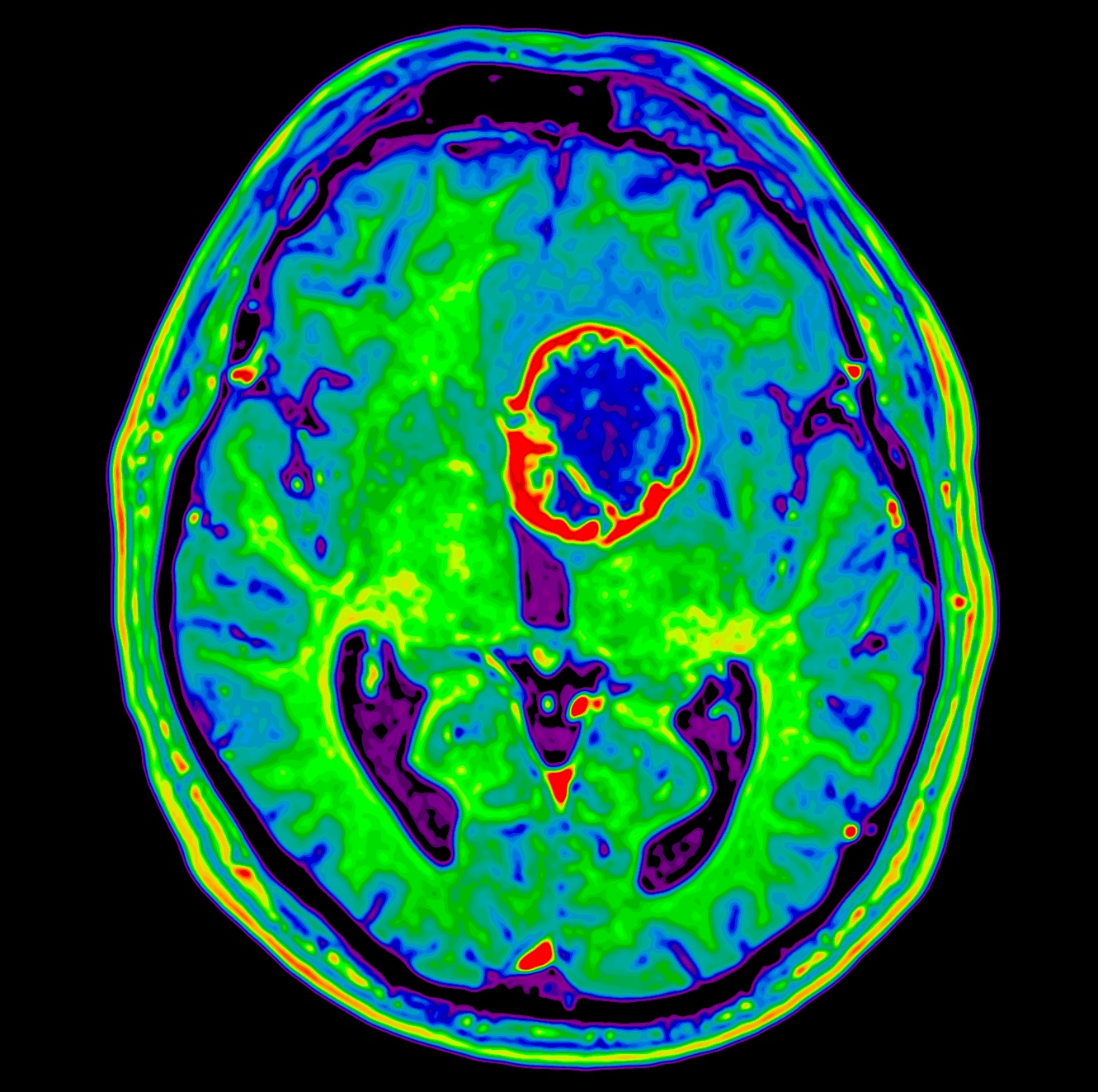
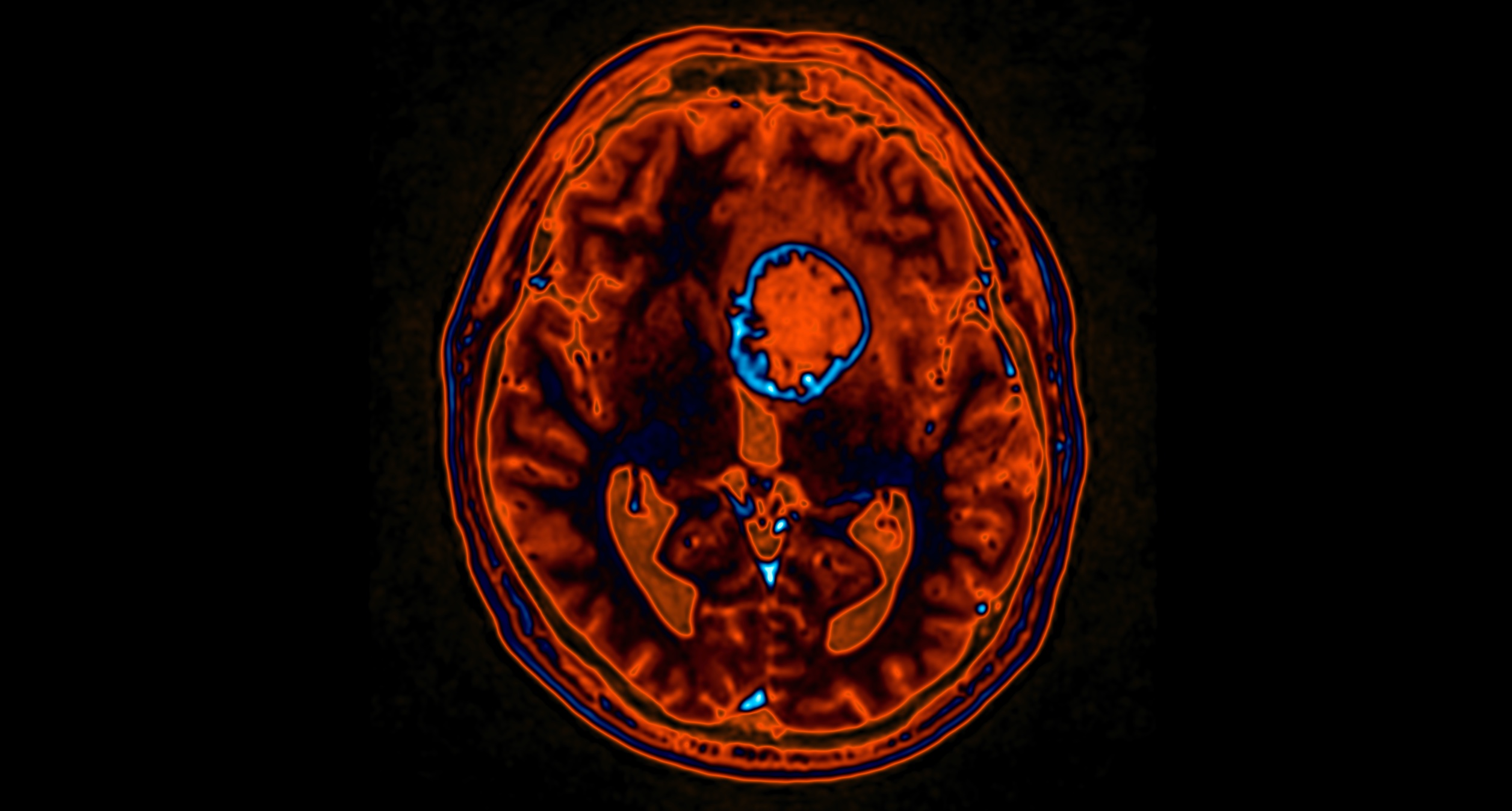
Top: T1 post-contrast with RANO bidimensional calipers (4.25 × 3.91 cm) — the codified RANO 2.0 endpoint. Same slice crossfaded with rCBV perfusion — adjunctive imaging where the criteria point but don't yet mandate. Bottom: 3D volumetric rotation across all slices.
Full-Stack Imaging
Why Volumetryx
RANO 2.0 codified volumetric as a co-equal method. The operational guide recommends consistent software across all patients. We made it our default. Bidimensional delivered when your protocol specifies it.
Pericavity rim or measurable nodule? Meningeal scar or enhancing tumor? These calls require neuro-oncology training. Our readers have it. Not generalists rotating across tumor types.
Median survival 14–16 months. A week-long read delay is not minor. 24–72h per timepoint read — workflow SLA, not aspiration.
BioSUITE runs two QA gates. First at the site, before submission — non-compliant acquisitions flagged while the patient is still available for re-scan. Second on receipt, before the reader opens the case. Resolution, parameter matching, sequence completeness validated twice. Nothing reaches the reader unchecked.

Any timepoint. Any protocol. We'll run a full volumetric analysis on your existing imaging and show you what your current reads are missing.